




Sinonasal Tumor is rare (estimated to occur in less than 1 in 100,000 individuals), and is twice more common in males than in females. Given the close proximity of the sinus and nasal cavities to the brain and orbits, it is vital to diagnose and treat these lesions as early as possible in order to avoid significant morbidity such as intracranial spread and vision loss. This post describes the symptoms that suggest the need for careful clinical evaluation, as well as the pertinent anatomy, diagnostic approach, and treatment options for the more common sinonasal tumors.

Contents
Symptoms of Sinonasal Tumors
Most sinonasal tumors are unilateral (one-sided), and cause symptoms that begin primarily on one side. These symptoms may include nasal obstruction (which can progress to cause blockage of both nasal cavities in the case of large tumors), nosebleeds, neurologic deficits (numbness in the cheek and/or dentition, loss of smell, blurry or double vision), facial pain, discolored nasal drainage, headaches, and slowly progressive facial deformity (eye protrusion, cheek or forehead swelling, widening or enlargement of the nasal dorsum). Rarely, malignant tumors may spread to lymph nodes in the neck and present initially as a neck mass.
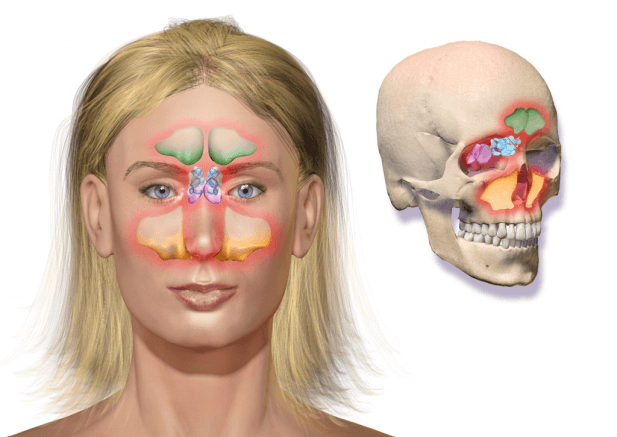
The Anatomy of Sinonasal Tumors
Sinonasal tumors most often arise from the maxillary sinus (~ 55%), followed by nasal cavity (~ 35%) and ethmoid sinus (~ 9%). The remainder of lesions are found in the frontal and sphenoid sinuses. Lesions within the nasal cavity have a 50:50 chance of being malignant, whereas tumors of the maxillary, ethmoid, frontal, and sphenoid sinuses are more often malignant than benign. Location also determines the risk of invasion into the adjacent structures. Lesions in the maxillary sinus may invade nearby nerves, blood vessels, and chewing muscles. Nasal cavity, ethmoid, sphenoid, and frontal sinus tumors often invade the skull base, resulting in intracranial extension that requires the expertise of skull base surgeons for adequate resection. In many cases, this can be safely achieved endoscopically without the need for external incisions or scars.
Getting A Diagnosis
Patients with symptoms concerning for sinonasal tumors need careful clinical examination including nasal endoscopy. Many lesions can be biopsied in the clinic setting with minimal discomfort for pathologic diagnosis (this often helps determine if the lesion is malignant versus benign and the nature of the tumor helps guide treatment decisions). Some lesions, particularly those that appear highly vascular and at risk for significant bleeding, must be biopsied in the operating room under anesthesia. Imaging (CT, MRI, and PET scan) is essential to determine the stage of the tumor, decide if and how it is resectable, and evaluate for metastases to lymph nodes in the neck or other common sites such as the lungs. CT scans aid in the initial evaluation for a mass and provide the best visualization of bony destruction, a common finding particularly for malignant lesions. MRI provides a much better view of the soft tissues, and is particularly important in the workup of lesions that invade intracranially or along nerves. PET scans are reserved for confirmed malignancies, and specifically evaluate for metastatic lesions in the neck and elsewhere in the body.
Treatment Options For Sinonasal Tumors
Many factors must be considered when determining the optimal treatment for patients with sinonasal tumors. Benign lesions often respond to complete surgical resection, and in most cases this can be accomplished endoscopically (without any external incisions, scars, or deformities). Malignant lesions must be staged, and lesions that have distant metastases (lungs, bone, brain, etc.) are generally considered poor candidates for surgery. Malignant lesions without distant metastases usually require surgical resection for the best chance of curing the disease. Surgery is done either endoscopically or through open approaches, depending upon the location and extent of the tumor. Radiation therapy with or without chemotherapy is an alternative to surgery in some cases, and is often recommended after surgery to increase chances for cure in advanced tumors with a high risk of recurrence. Lymph node metastases in the neck require a neck dissection for removal, which involves a separate incision on one or both sides of the neck. While surgical resection often involves the sacrifice of nerves, blood vessels, and functional tissues to ensure adequate margins and complete removal of the tumor, the anticipated postoperative functional deficits are different for every patient depending on the size, location, and invasiveness of their tumor.
Why Choose Dr. Kuperan For Endoscopic Resection
Dr. Kuperan with Houston Advanced Nose & Sinus has trained extensively in endoscopic resection of sinonasal tumors and skull base surgery, and provides academic-level care with the convenience of a private practice setting. Sinonasal tumors are rare, and in most cases surgery provides the best chance of curing the disease. If you or someone you know has symptoms concerning for a sinonasal tumor, do not wait to seek an evaluation as tumors often progress rapidly once symptoms arise. Click here to schedule a consultation today.